Metal split piece causes penetrating injury that mimics gun shot injury: Case Report

A metal split piece penetrated the left supraclavicular region of 27 year's old Arabic man mimicking a gun bullet, according to a case study published in the Journal of Medical Case Reports. What is surprising about this case is that the man was fully conscious, oriented, and hemodynamically stable after the accident.
According to the case study, the man was presented to the emergency department of Isola d’Elba Hospital 1 hour after an occupational hazard occurred while he was making firewood with an axe for the wood oven of his restaurant. He stated that a metal sliver, coming from the axe using for wood chopping, penetrated his neck in the left supraclavicular region. On admission, he was fully conscious, oriented, and hemodynamically stable. He did not refer to a significant past medical history.
His vital parameters were normal: his pulse rate was 70 beats per minute (bpm), his blood pressure was 140/80 mmHg, peripheral blood oxygenation was 95% without oxygen therapy, and the corporeal temperature was 36.3 °C. He also did not demonstrate any clinical symptoms such as chest pain or dyspnea: respiratory excursions were full and symmetrical, lungs resonant to percussion, and vesicular breath sound was reduced in left basal field; no rales, rhonchi, wheezes, or rubs were present; vocal and tactile fremitus was reduced in the same field. The results of a cardiovascular examination were: no abnormal heaves or lifts; no trill; regular rate and rhythm; no extra sounds or murmurs. At the level of his abdomen: no abnormal tympany was detected, with normal bowel sounds; superficial and deep palpation did not reveal any organomegaly or masses; no evidence of direct or rebound tenderness, rigidity, or guarding; liver and spleen appeared to be of normal size. At a neurological examination, he was alert and attentive.
His speech was clear and fluent with a good repetition, comprehension, and naming. There was no pronator drift of outstretched arms. His muscle bulk and tone were normal. Strength was full bilaterally. His reflexes were 2+ and symmetric at the biceps, triceps, knees, and ankles. Plantar responses were flexor. Light touch, pinprick, position sense, and vibration sense were intact in fingers and toes. Rapid alternating movements and fine finger movements were intact. There was no dysmetria on finger-to-nose and heel-knee-shin. There were no abnormal or extraneous movements. Romberg sign was absent.
On the basis of the collected anamnestic data, he underwent computed tomography (CT) scan that showed left hemopneumothorax, pneumomediastinum, and subcutaneous emphysema, without any signs of active bleeding. Another important radiological finding was the evidence of a metal foreign body in the left side of his chest cavity above the ipsilateral hemidiaphragm. No cervical structural injuries were detected upon radiological examination. A tube was placed in the left side of his chest with drainage of approximately 1000 mL of blood. He was then transferred by helicopter to our department in the Siena Hospital, tertiary trauma center, for the surgical removal of the foreign body. He was immediately brought to the operating room where he was intubated with a double-lumen endotracheal tube. Biportal video-assisted thoracic surgery (VATS) was performed: a 10 mm camera port was placed on the IX intercostal space, midaxillary line, and a 5 mm working port was made on the V intercostal space on the site of the chest tube, which was previously inserted.
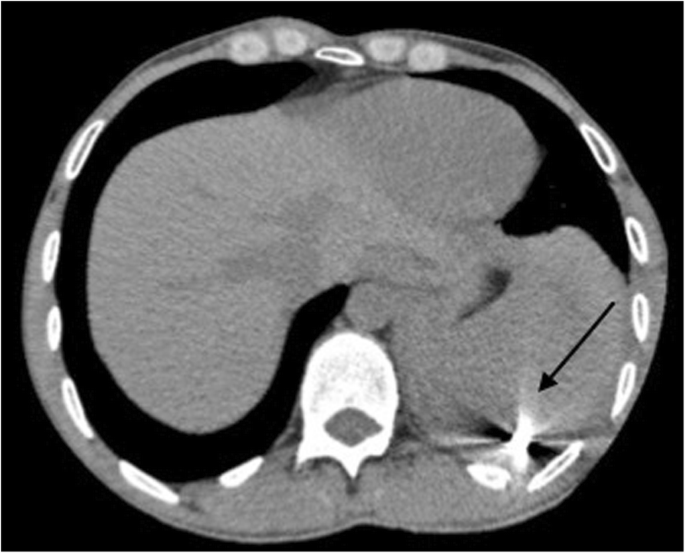 Chest computed tomography scan: evidence of a metal foreign body in the left chest cavity above the ipsilateral hemidiaphragm (the arrow indicates the metal foreign body)
Chest computed tomography scan: evidence of a metal foreign body in the left chest cavity above the ipsilateral hemidiaphragm (the arrow indicates the metal foreign body)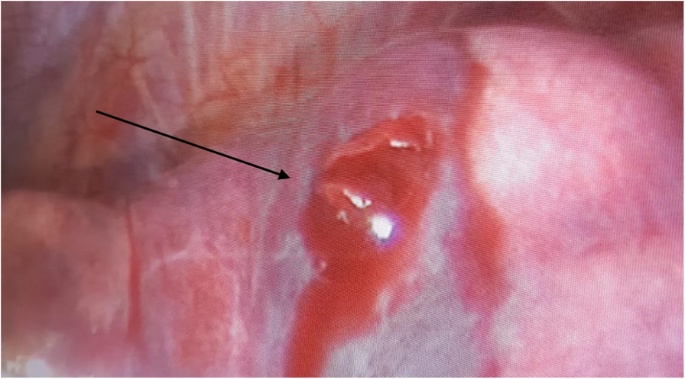 Lung injury: exit wound in the dorsal segment of the left upper lobe (the arrow indicates the exit wound)
Lung injury: exit wound in the dorsal segment of the left upper lobe (the arrow indicates the exit wound)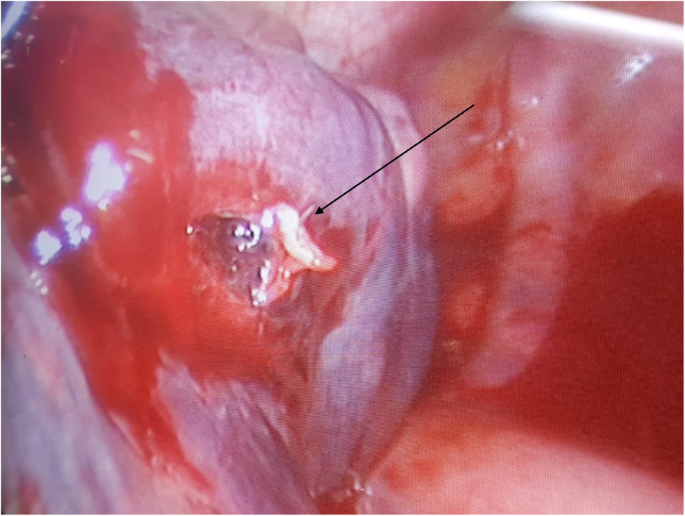 Lung injury: entrance hole at the left pleural dome (the arrow indicates the entrance hole)
Lung injury: entrance hole at the left pleural dome (the arrow indicates the entrance hole)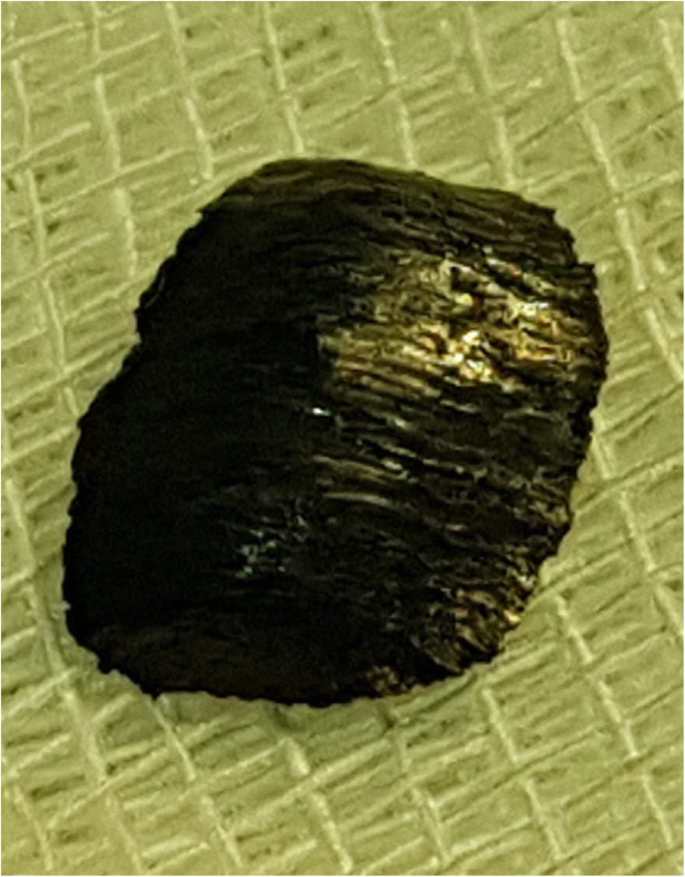 Foreign body: 1.5 cm pointed, sharp metal sliver
Foreign body: 1.5 cm pointed, sharp metal sliverLeft-sided VATS showed persistent hemothorax (600 mL) with blood clots that were removed. During the chest cavity inspection, the doctors found the foreign body, visible on the CT scan, in the left costodiaphragmatic angle. It consisted of a 1.5 cm pointed, sharp metal sliver, entering his supraclavicular region.
The authors concluded that the sliver narrowly missed the subclavian vessels, mimicking a gun bullet. In fact, while exploring his chest cavity, th authors noticed the entrance hole at the left pleural dome where the sliver had just penetrated the apex of the lung passing through the upper lobe of his left lung creating an exit wound in the dorsal segment of the same lobe.
"In the literature, there are several case series about this topic, with some of them reporting unusual foreign bodies that lead to penetrating trauma. However, to the best of our knowledge, no cases like the one we have reported are described in the current literature." concluded the authors.
For reference, click on the link
Journal of Medical Case Reports
Disclaimer: This site is primarily intended for healthcare professionals. Any content/information on this website does not replace the advice of medical and/or health professionals and should not be construed as medical/diagnostic advice/endorsement or prescription. Use of this site is subject to our terms of use, privacy policy, advertisement policy. © 2020 Minerva Medical Treatment Pvt Ltd