Coronary artery calcium scoring: On the rise but how reliable?

There is a steep rise in the burden of diabetes, obesity, and hypertension with prolongation of life expectancy. Thus ischemic heart disease is also prevalent and non-invasive testing is in demand. The technique of summing coronary calcium score (CAC) by Agatston is the most widely used.Grouping can be done as - Absence of calcification; minimal calcification (1-10); mild (11-100); moderate (101-400); severe (401-1000); and extensive (more than 1000).
Calcium score zero!
Absence of calcium in the coronary arteries does not mean absence of atherosclerosis, as there may be non-calcified plaques.
Coronary artery calcification (CAC) demonstrated by multi-detector computed tomography (MDCT) was compared with myocardial perfusion assessed by cardiac magnetic resonance imaging (CMR) in a group of symptomatic patients. A group of 120 patients was divided on presence or absence of high grade (HG) stenosis.The CAC score was lower in patients with no-HG stenosis compared to those with HG stenosis with the statistically significant p-value. The role of CAC scoring was more important in excluding cardiac perfusion abnormalities i.e. specificity was more than sensitivity.
In patients with no stenosis, the incremental relationship between coronary calcium score and the extent of myocardial perfusion suggests coronary wall hardening as an additional mechanism for stress-induced angina other than luminal narrowing. These findings could be clinically useful in treatment planning of such patients other than existing ones according to authors.
They also concluded that coronary calcium score remains more accurate in detecting HGluminal stenosis over and above myocardial perfusion defects by CMR.
Myocardial perfusion scintigraphy does not detect the disease without flow restriction, exposes the patient to high levels of radiation and is costly. Contrary to this, with less radiological exposure, calcium score is directly correlated to the presence and extension of coronary atherosclerosis. (Source: Siqueira et al in an article on Relationship between calcium score and Scintigraphy, 2016) Scintigraphy however, scored over calcium scoring in acute ischemic events.
Few articles have tried establishing a correlation between CAC score and rest-stressPET (Positron emission tomography) or SPECT (single photon emission computed tomography) imaging in patients with suspected coronary artery disease. A study by Hoang Lai et al in 2011 concluded-
Patients with moderate or severe LCX or RCA ischemia have significantly higher CAC scores than those with no or mild ischemia. Patients with moderate or severe LAD ischemia have insignificantly higher CAC scores than those with no or mild ischemia.
CAC scoring has a complementary role with CT/MR myocardial perfusion techniques.Coronary angiography is better for estimation of stenosis. ‘’Vulnerable plaques on CTCA, even those that were normal on myocardial perfusion image, were associated with future ACS events’’- thus assessment of plaque-type being important in future. Source: Lei Xu, Zhonghua Sun, and Zhanming Fan, “Non-invasive Physiologic Assessment of Coronary Stenosis Using Cardiac CT,” BioMed Research International, 2015.
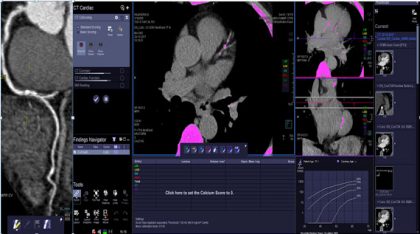
Coronary artery scoring, measuring plaque and summation planning by automated software at our institute
Dr. Niharika Prasad,
The author is MD (Radiodiagnosis) and is Senior Resident, Dept of Radiology in All India Institute of Medical Sciences, AIIMS Patna. She is a member Editorial Board, Radiology at Specialty Medical Dialogues.
Disclaimer: This site is primarily intended for healthcare professionals. Any content/information on this website does not replace the advice of medical and/or health professionals and should not be construed as medical/diagnostic advice/endorsement or prescription. Use of this site is subject to our terms of use, privacy policy, advertisement policy. © 2020 Minerva Medical Treatment Pvt Ltd