Choledocholithiasis /Gall Stones-Standard Treatment guidelines
Introduction
Choledocholithiasis is suspected in patients presenting with colicky upper abdominal pain that may or may not radiate to back (biliary colic). This may be associated with jaundice. About 8-20% of patients who have gallbladder stones were found to have choledocholithasis in published literature1 . About 5% of common bile duct stones found during an operation may be unsuspected preoperatively2 .
Ministry of Health and Family Welfare, Government of India has issued the Standard Treatment Guidelines for Choledocholithiasis.
Following are the major recommendations :
Case definition
Choledocholithiasis is occurrence of stones within the common bile duct or common hepatic duct.
INCIDENCE OF THE CONDITION IN OUR COUNTRY
Published data on the incidence of choledocholithiasis is limited.
DIFFERENTIAL DIAGNOSIS
a.Gallbladder stone disease
b.Mirrizzi syndrome
c.Choledochal cyst
d.Benign biliary stricture
e.Malignant obstruction of extra-hepatic biliary tree
PREVENTION AND COUNSELING
No specific primary or secondary preventive measures are known.
OPTIMAL DIAGNOSTIC CRITERIA, INVESTIGATIONS, TREATMENT AND REFERRAL CRITERIA
History: Abdominal pain is the most common symptom. Jaundice with or without cholestatic features like pruritus and clay colored stools, fever with chills due to cholangitis, acute pancreatitis may also form part of history.
(Physical examination is usually non-contributory).
Diagnosis: Elevated levels of serum bilirubin and alkaline phosphatase indicate biliary obstruction but are not sensitive or specific for choledocholithiasis. Normal levels of bilirubin, alkaline phosphatase or liver enzymes like aspartate transaminase and alanine transaminase will not rule out choledocholithiasis.
Ultrasound scan abdomen is usually the first imaging modality to raise the suspicion of choledocholithiasis. Sensitivity and specificity of ultrasound scan for diagnosis are 30% and close to 100% respectively3. Magnetic resonance cholangio pancreatography (MRCP) has demonstrated sensitivity and specificity of 91% and 100% respectively. Sensitivity of MRCP decreases to about 71% for stones less than 5 mm4. Endoscopic ultrasound (EUS) scan of bile duct has been shown to have sensitivity and specificity of 84-100% and 96-100% respectively. Positive predictive values of MRCP and EUS for diagnosis were 0.87 and 0.93 respectively. Corresponding negative predictive values were 0.92 and 0.96. All these are in comparison to endoscopic retrograde cholangio pancreatography (ERCP) which has been given up as a diagnostic modality. It is currently recommended only for therapeutic use to remove bile duct stone after a reasonable diagnosis of choledocholithiasis has been arrived at.
Treatment
In patients who have undergone cholecystectomy earlier and diagnosis of choledocholithiasis, endoscopic retrograde cholangio pancreatography (ERCP) and extraction of bile duct stones using endoscopic techniques is the preferred approach. If this fails, open or laparoscopic common bile duct exploration should be performed. A possibility that dilated common bile duct with calculi is a choledochal cyst must be kept in mind as treatment & long term follow up of the latter is different.
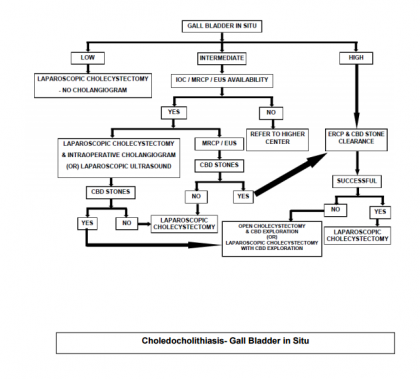
In patients with gall bladder stones and high risk of choledocholithiasis, ERCP and stone retrieval followed by laparoscopic cholecystectomy is the preferred treatment. If endoscopic therapy fails, they may undergo laparoscopic or open common bile duct exploration along with cholecystectomy.
A cautious decision to withhold cholecystectomy after endoscopic treatment of choledocholithiasis may be made in patients with unacceptable surgical risk.
If there is intermediate risk of choledocholithiasis in those with gallstones this should be confirmed with MRCP or EUS. Thereafter treatment is as outlined above.
Patients with low risk of choledocholithiasis and gallstones may undergo intraoperative cholangiogram (IOC). If choledocholithiasis if diagnosed, and the bile duct is of normal caliber, exploration is not advised. Post operative endoscopic therapy is an option. If the common bile duct is dilated options are: laparoscopic common bile duct exploration / conversion to open operation and common bile duct exploration.
Patient must be referred to higher centers if either of MRCP, EUS or intraoperative cholangiogram facilities are unavailable.
Situation 1
At secondary hospital / non-metro situation: optimal standards of treatment in situations where technology and resources are limited
Clinical diagnosis
The most common presentation is with colicky upper abdominal pain (biliary colic) with or without jaundice. Fever with chills would indicate cholangitis. Pruritus and clay colored stools may be present if biliary obstruction is high grade. Fever and icterus may be present on general examination. There are no specific abdominal signs that would indicate choledocholithiasis. Presence of distended gallbladder will be a pointer against the diagnosis of choledocholithiasis in most cases.
Investigations
Haemogram, liver function test, ultrasound scan abdomen. MRCP should preferably be available even in this situation.
Case definition
Choledocholithiasis is occurrence of stones within the common bile duct or common hepatic duct.
Treatment
We recommend two treatment protocols depending on whether cholecystectomy has been performed earlier. These protocols have been given in the form of two algorithms along with this document. It would be acceptable not to have high end technology like endoscopic ultrasound scan (EUS), laparoscopic ultrasound scan or instrumentation for laparoscopic common bile duct exploration in a secondary referral hospital setting.
Standard operating procedure (please see the two algorithms)
Most of the investigations may be performed as an outpatient. Cholangitis would make admission mandatory during the initial evaluation itself.
Referral criteria
Patients with cholangitis unresponsive to antibiotic therapy should be referred to a tertiary (super specialty) hospital. Patients with failed papillary access / biliary cannulation (at ERCP and attempt at stone extraction) should also be considered for referral to tertiary care centers before decision to perform open common bile duct exploration.
Situation 2
At super specialty facility in metro location where high end technology is available
Clinical diagnosis
Careful review of symptoms and signs must be done.
Investigations:
If cholangitis was the indication for referral, complete blood count, coagulation profile and blood culture and sensitivity must be done at admission. Liver function tests and ultrasound scan abdomen to confirm the diagnosis and to look for cholangitic abscess should be performed. Parenteral vitamin K supplementation must be initiated during the period of evaluation. After initiation of appropriate antibiotic therapy, it may be reasonable to proceed to ERCP and attempt at endoscopic retrieval of bile duct stones.
Treatment:
Our suggested treatment protocol is in the form of algorithms attached with this document.
Standard Operating procedure
All investigations can be done as outpatient/day care procedures. However, if cholangitis is present, patient should be hospitalized.
All surgical procedures require hospitalization.

Guidelines by The Ministry of Health and Family Welfare :
Anand Bharathan
V Sitaram
Department of Hepatic Pancreatic & Biliary (HPB) Surgery
Christian Medical College
Vellore.
Next Story
Disclaimer: This site is primarily intended for healthcare professionals. Any content/information on this website does not replace the advice of medical and/or health professionals and should not be construed as medical/diagnostic advice/endorsement or prescription. Use of this site is subject to our terms of use, privacy policy, advertisement policy. © 2020 Minerva Medical Treatment Pvt Ltd