Balloon choice for PCIs in calcific lesions - Dr M G Pillai

In the last two decades, we have seen a substantial increase in the number of PCIs and extremely complex, calcific coronary lesions are being treated with dexterity using various debulking devices. As per ACC/AHA, an inclining trend towards the prevalence of type C lesions and severity of calcium deposits in coronary arteries is also observed. The spectrum of calcified coronaries is also varying pathologically and anatomically.
Approach to the lesion preparation: The methodology depends upon the severity of calcium and tortuosity.
Imaging modalities: IVUS and OCT has an added advantage for assessment of the lesion and final optimization of procedure resulting in excellent long term results.
The success of a procedure depends on choice of debulking devices and today I am discussing my balloon choice in calcific lesions. The balloon catheter must have a deliverability, crossability and must safely open the target.
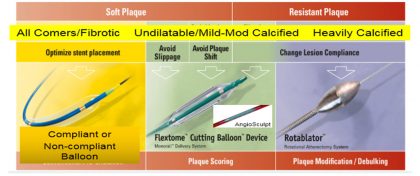
NC balloons are the workhorse of today for all lesions in general. These balloons have the characteristics of not having the Dog Bone effect and they withstand/delivers high pressure and it cracks heavily calcified lesion. However, they are less trackable through vasculature.

Cutting balloons incise the coronary atheroma during the inflation by the help of 3-4 sharp micro blades mounted in a non-compliant balloon. This results in controlled micro incisions in the atheromatous plaque at a lower to moderate pressure. It prevents the longitudinal tears, reduces the vessel stress/injury and achieves larger lumen.
![]()
Scoring balloon is an alternative to cutting balloon containing 3 spiral struts of nitinol ribbon to incise the atheromatous plaque. It has minimal slippage with less flow limiting dissections. Unlike cutting balloon, it shaves off the plaque in a circumferential manner.
Lesion characteristics confirmed on IVUS/OCT dictates the option of NC Balloon / Cutting / Scoring or newer devices.
There are few reports of High-pressure NC balloons (>30 ATM), however, I believe these may result in barotrauma to vessels resulting in aggressive restenosis.
The author, Dr. Madhavan Govinda Pillai (M.G. Pillai) is a Senior Interventional Cardiologist, Prof. & Head of Cardiology at Nanavati Super Speciality Hospital, Mumbai. He is presenting a lecture on the topic "My balloon choice in calcified lesion debulking Non compliant / cutting / scoring"at India Live 2018.
Disclaimer: This site is primarily intended for healthcare professionals. Any content/information on this website does not replace the advice of medical and/or health professionals and should not be construed as medical/diagnostic advice/endorsement or prescription. Use of this site is subject to our terms of use, privacy policy, advertisement policy. © 2020 Minerva Medical Treatment Pvt Ltd