Management of unanticipated difficult tracheal intubation in obstetrics: 2016 guidelines
Management of unanticipated difficult tracheal intubation in obstetrics: All India Difficult Airway Association 2016 guidelines
The various physiological changes in pregnancy make the parturient vulnerable for early and rapid desaturation. Severe hypoxaemia during intubation can potentially compromise two lives (mother and foetus). Thus tracheal intubation in the pregnant patient poses unique challenges, and necessitates meticulous planning, ready availability of equipment and expertise to ensure maternal and foetal safety.
The All India Difficult Airway Association (AIDAA) proposes a stepwise plan for the safe management of the airway in obstetric patients. These were published in the Indian Journal of Anaesthesia, Volume 60, Issue 12, 09 Dec 2016.
These guidelines have been developed based on available evidence; wherever robust evidence was lacking, recommendations were arrived at by consensus opinion of airway experts, incorporating the responses to a questionnaire sent to members of the AIDAA and the Indian Society of Anaesthesiologists (ISA). Following are the major recommendations:
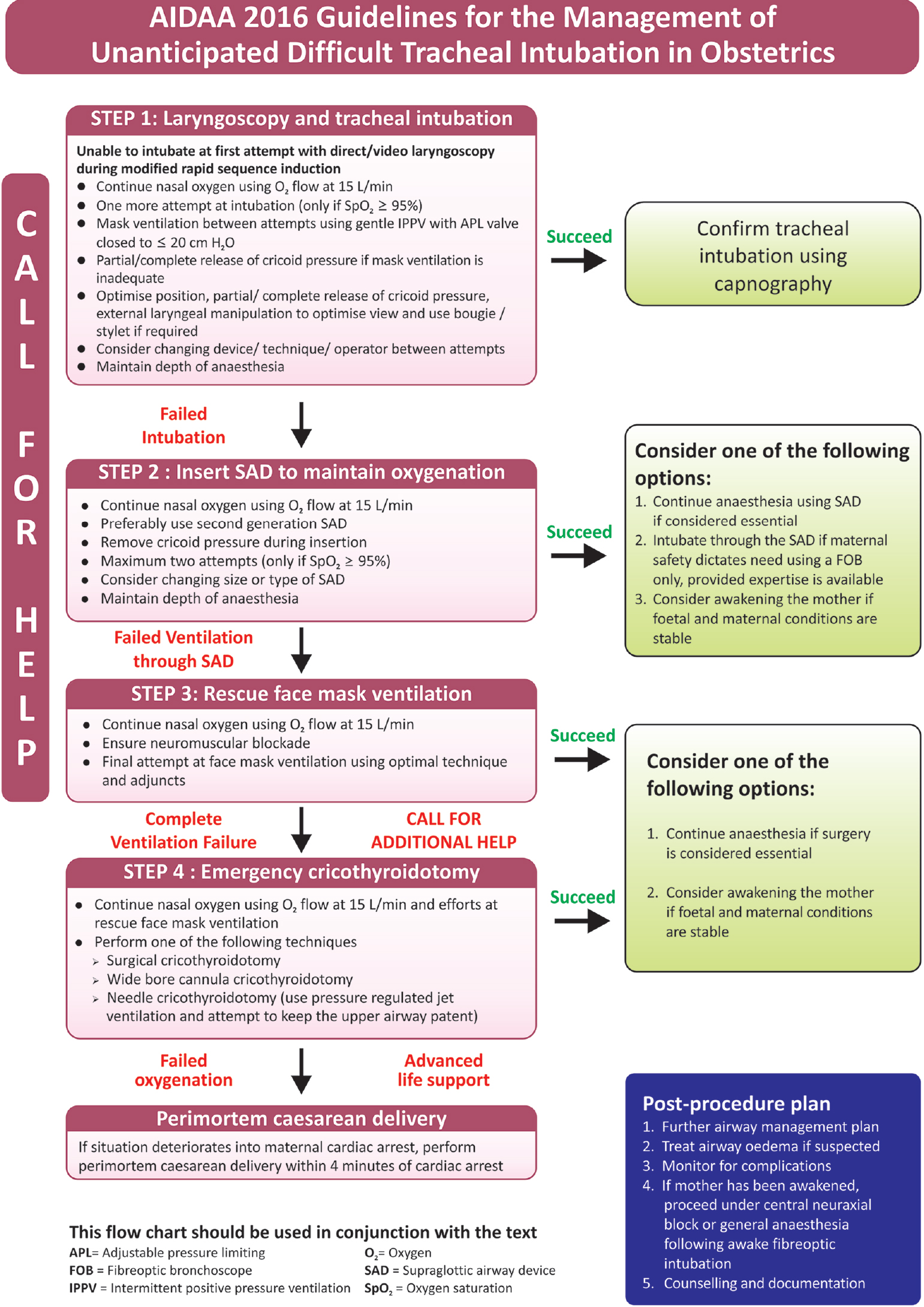
Stepwise approach to management of unanticipated difficult intubation in obstetrics
Step 1
When intubation is successful at first laryngoscopy, the obstetrician proceeds to deliver the infant. However, if the first attempt at intubation fails, the anaesthesiologist should 'Call for help' immediately and focus on reoxygenation. Bag-mask ventilation with the APL valve set to ≤20 cm H 2 O should be resumed, preferably a two-handed two-person technique with use of airway adjuncts such as an oropharyngeal or nasopharyngeal airway as deemed appropriate. The anaesthetic assistant should be instructed to release the cricoid pressure in a graded manner while the first anaesthesiologist constantly checks the ability to ventilate. Should bag-mask ventilation prove successful, the anaesthesiologist should attempt a second laryngoscopy after optimising head/neck position and releasing the cricoid pressure in a graded manner. The second attempt at laryngoscopy should be performed using a videolaryngoscope, alternate blades and use of a bougie as dictated by availability of equipment and expertise. A videolaryngoscope provides an additional advantage to the assistant who can now release the cricoid pressure in a graded manner while observing the impact on laryngoscopic view. Should the second attempt at intubation be successful, the obstetrician proceeds to deliver the infant. However, should this attempt also fail, this is now a 'failed intubation' and one should proceed to Step 2.
Step 2
While nasal oxygen continues to be administered at 15 L/min, the anaesthesiology team now focuses attention on placing a SAD to facilitate anaesthesia and oxygenation. A maximum of two attempts may be allowed in placing a second generation SAD with graded release of cricoid pressure as described earlier. Once the SAD is properly placed, the team proceeds depending on the foetal and maternal condition. If the indication for caesarean delivery was a nonreassuring foetal status, the obstetrician proceeds to deliver the infant with anaesthesia being continued through the SAD despite a definite albeit low risk of pulmonary aspiration. Once the foetus is delivered, the anaesthesiologist may consider intubating through the SAD should maternal haemorrhage, imminent seizures and high risk for aspiration exist. Intubation through the SAD should be done only using fibreoptic bronchoscopy provided expertise is available.
On the other hand, if foetal and maternal conditions are stable (not warranting immediate delivery of the infant), the team is advised to awaken the mother. The anaesthesiologist can then consider performing caesarean delivery under central neuraxial block or GA following awake fibreoptic-aided intubation. Should placement of a SAD fail after 2 attempts, this is now a 'failed ventilation through supraglottic airway device' and one should proceed to Step 3.
Step 3
While nasal oxygen continues to be administered at 15 L/min, one final attempt is made at rescue face mask ventilation using optimal technique and airway adjuncts as deemed appropriate. The anaesthesiologist should ensure that neuromuscular blockade is adequate before making this final attempt at face mask ventilation. Should this also fail, the situation is now that of a 'complete ventilation failure' and the anaesthesiologist should seek urgent expert assistance.
Step 4
This situation of complete ventilation failure is serious and demands emergent management. The team should 'Call for additional help' and start positioning the patient for emergency cricothyroidotomy. Based on the availability of equipment and expertise, the team can opt for one of the following three options - a surgical cricothyroidotomy, wide bore cannula cricothyroidotomy or needle cricothyroidotomy (with concomitant use of pressure-regulated jet ventilation while maintaining patency of the upper airway). As outlined before, the maternal and foetal condition will determine whether the team proceeds to deliver the infant or awaken the mother.
Failure of emergency cricothyroidotomy can potentially deteriorate into a maternal cardiac arrest. In the unfortunate event of a maternal cardiac arrest, cardiopulmonary resuscitation in the form of chest compressions is continued with another team member providing left uterine displacement. Perimortem caesarean delivery performed within 4 minutes of cardiac arrest could enhance chances of foetal survival.
Although a number of guidelines from various countries exist, AIDAA has embarked on this endeavour to formulate guidelines of our own keeping in mind the infrastructure and varying standard of care at different healthcare set-ups in our country.
Indian guidelines specially emphasise:
- SpO 2 of equal to or more than 95% as a cut-off for escalating airway interventions
- Limiting the number of intubation attempts to two before proceeding to the next step
- Continuous administration of nasal oxygenation through nasal cannula to prolong apnoea time
- We also aim to enforce a minimum standard of care through these guidelines (such as, for instance, confirmation of tracheal intubation by ETCO 2 monitoring).
Extubation
Every extubation should be considered as a potential reintubation, and this is especially true when extubating a difficult airway. A planned extubation strategy should be ready before extubating a difficult airway. AIDAA guidelines for extubation deal with strategising extubation and other advance methods of extubation which can be applied in the obstetric scenario as well.
Following is the algorithm suggested by AIDAA for the management of Unanticipated difficult tracheal intubation :
{kind=link}
Image Source: All India Difficult Airway Association, Guidelines published in Indian Journal of Anesthesiology Volume 60,Issue 12, Dec 2016
You can read the article by clicking on the following link:
http://www.ijaweb.org/article.asp?issn=0019-5049;year=2016;volume=60;issue=12;spage=899;epage=905;aulast=Ramkumar
The guidelines issued by AIDAA 2016 are featured in the December issue of Indian Journal of Anesthesia:
http://www.ijaweb.org/
Our comments section is governed by our Comments Policy . By posting comments at Medical Dialogues you automatically agree with our Comments Policy , Terms And Conditions and Privacy Policy .
Disclaimer: This site is primarily intended for healthcare professionals. Any content/information on this website does not replace the advice of medical and/or health professionals and should not be construed as medical/diagnostic advice/endorsement or prescription. Use of this site is subject to our terms of use, privacy policy, advertisement policy. © 2020 Minerva Medical Treatment Pvt Ltd